Key takeaways
- A patient with hemorrhagic radiation proctitis continued to bleed despite argon plasma coagulation, bipolar cautery, sucralfate enemas, mesalamine suppositories, and radiofrequency ablation.
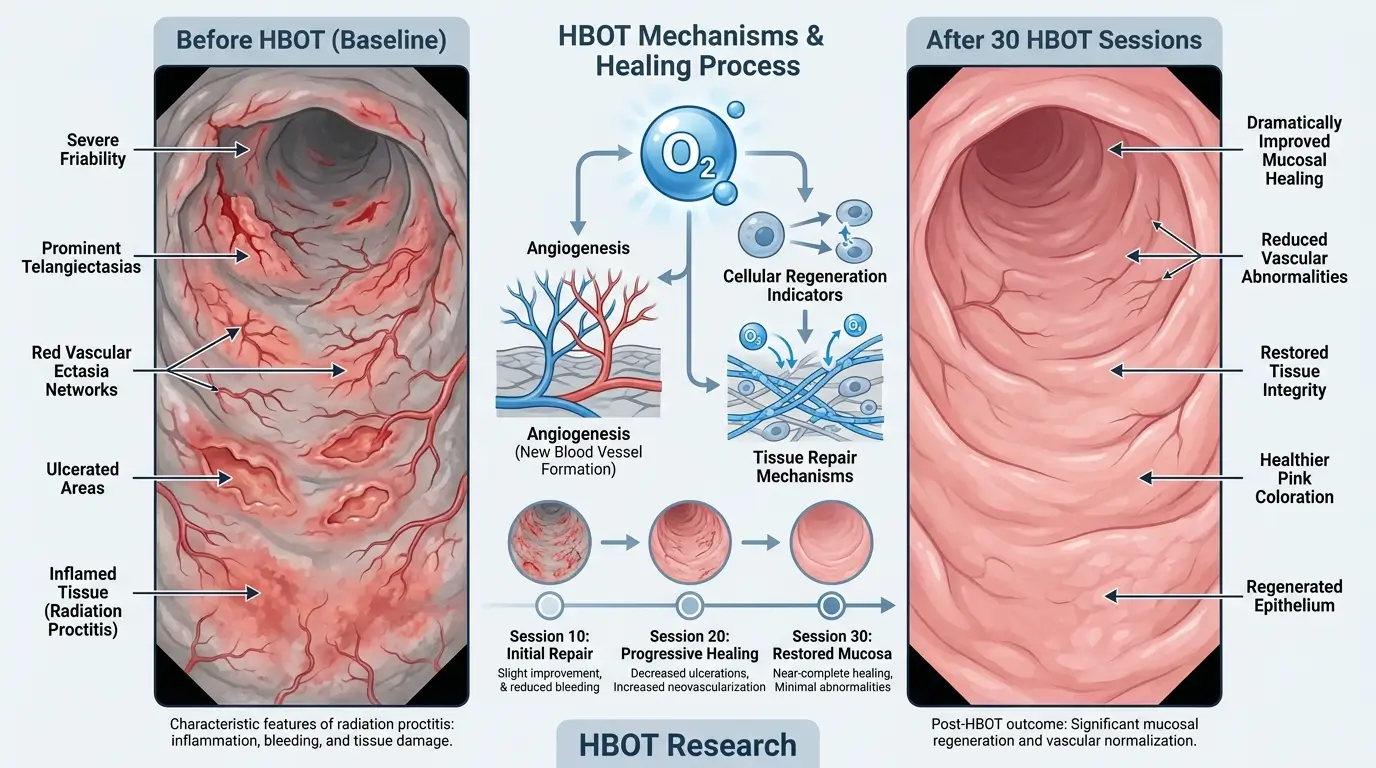
- He completed 30 hyperbaric oxygen sessions over seven weeks.
- Rectal bleeding resolved completely after hyperbaric oxygen therapy.
- Follow-up sigmoidoscopy showed resolution of radiation proctitis with one clean-based ulcer.
- Hyperbaric oxygen improves tissue oxygenation, stimulates angiogenesis, and aids healing in irradiated rectal tissue.
Radiation proctitis developed years after pelvic radiation for prostate cancer.
Chronic radiation proctitis causes rectal bleeding, urgency, and anemia in some patients. Standard treatments focus on endoscopic ablation or topical agents. When bleeding persists, options narrow. This case shows one pathway that succeeded where others failed.
What is chronic radiation proctitis?
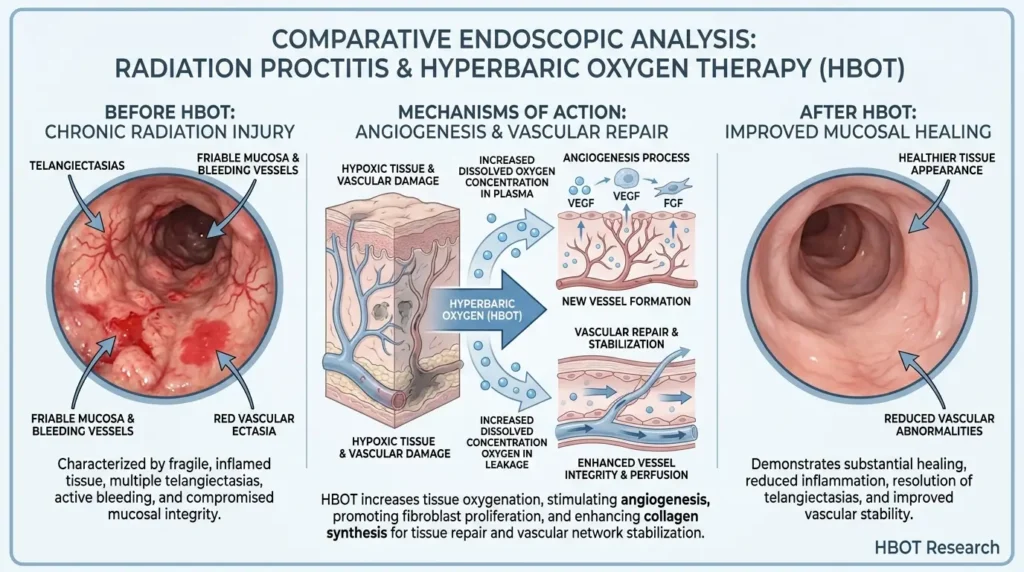
Radiation proctitis is inflammation and ischemia of the rectal lining after radiation therapy for pelvic cancers. Acute cases occur during or soon after treatment and often resolve. Chronic cases appear months or years later. They feature telangiectasias, ulcers, fibrosis, and bleeding.
Why does bleeding continue after endoscopic treatment?
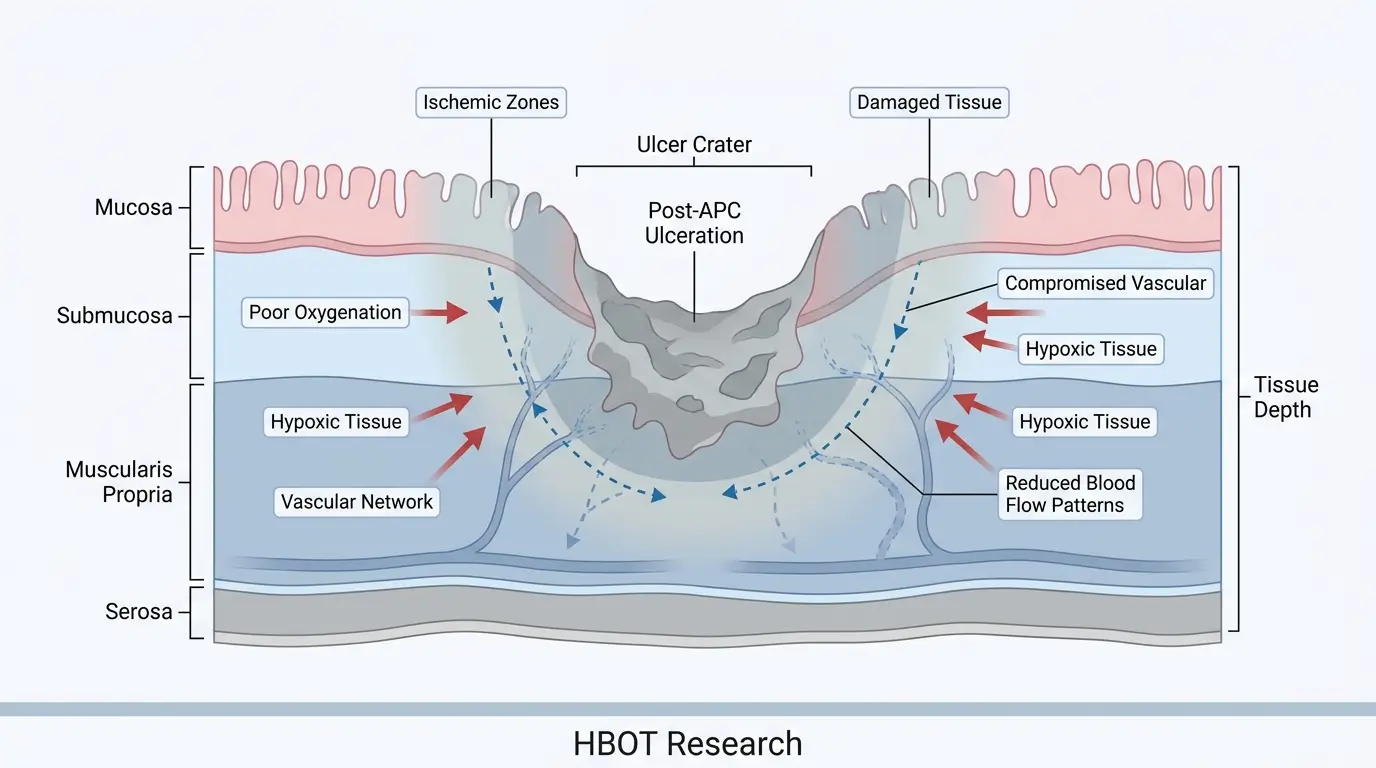
Repeated argon plasma coagulation can create ulcers in already damaged tissue with poor blood supply. The patient required three APC sessions, then bipolar electrocautery for visible vessels in post-treatment ulcers. Sucralfate enemas reduced bleeding temporarily. Mesalamine and radiofrequency ablation followed, yet intermittent bleeding remained.
When do doctors turn to hyperbaric oxygen therapy?
Physicians consider hyperbaric oxygen when bleeding continues despite topical agents and multiple endoscopic interventions. In this case, ongoing symptoms after radiofrequency ablation prompted referral. The patient received 30 sessions across seven weeks.
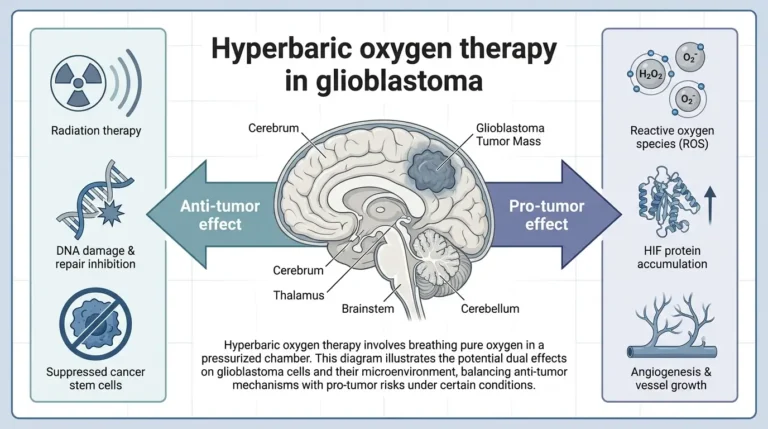
How does hyperbaric oxygen therapy work in radiation injury?
Hyperbaric oxygen delivers 100 percent oxygen at elevated pressure. It raises oxygen levels in hypoxic tissue, promotes new blood vessel growth, and supports mucosal repair. The authors note this mechanism addresses the underlying endarteritis and impaired healing caused by radiation.
What were the results in this patient?
Bleeding stopped after the course of hyperbaric oxygen. Follow-up flexible sigmoidoscopy confirmed healed radiation proctitis with only one clean-based ulcer. Biopsies ruled out infection or dysplasia. Mesalamine was discontinued.
What barriers limit wider use of hyperbaric oxygen?
Access to chambers, high cost, insurance approval, and the demand for 30 or more sessions create practical hurdles. These factors often delay or prevent treatment even when clinically appropriate.
Why this matters
This stepwise case illustrates that refractory hemorrhagic radiation proctitis often requires multimodal care. It provides concrete evidence that hyperbaric oxygen can succeed after endoscopic and topical options fall short. Clinicians now have clearer guidance on when to escalate to HBOT.
References
- Cureus, “Refractory Hemorrhagic Radiation Proctitis Managed With Sequential Endoscopic, Topical, and Hyperbaric Oxygen Therapy”, 2024, https://www.cureus.com/articles/507611-refractory-hemorrhagic-radiation-proctitis-managed-with-sequential-endoscopic-topical-and-hyperbaric-oxygen-therapy