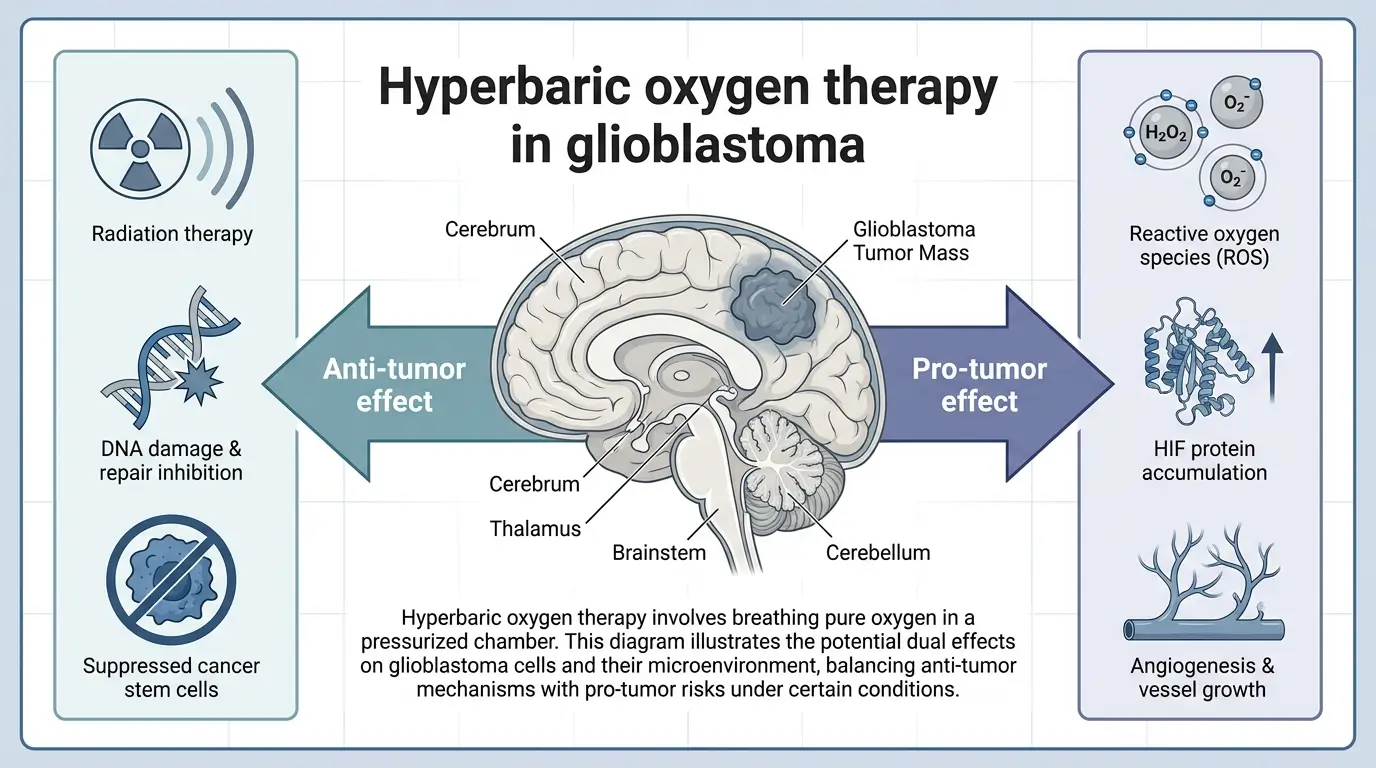
- A peer-reviewed mini-review concludes hyperbaric oxygen therapy has both anti-tumor and pro-tumor effects in glioblastoma.
- The therapy can raise oxygen levels in tumor tissue by 100 to 115 percent, increasing damage from radiotherapy.
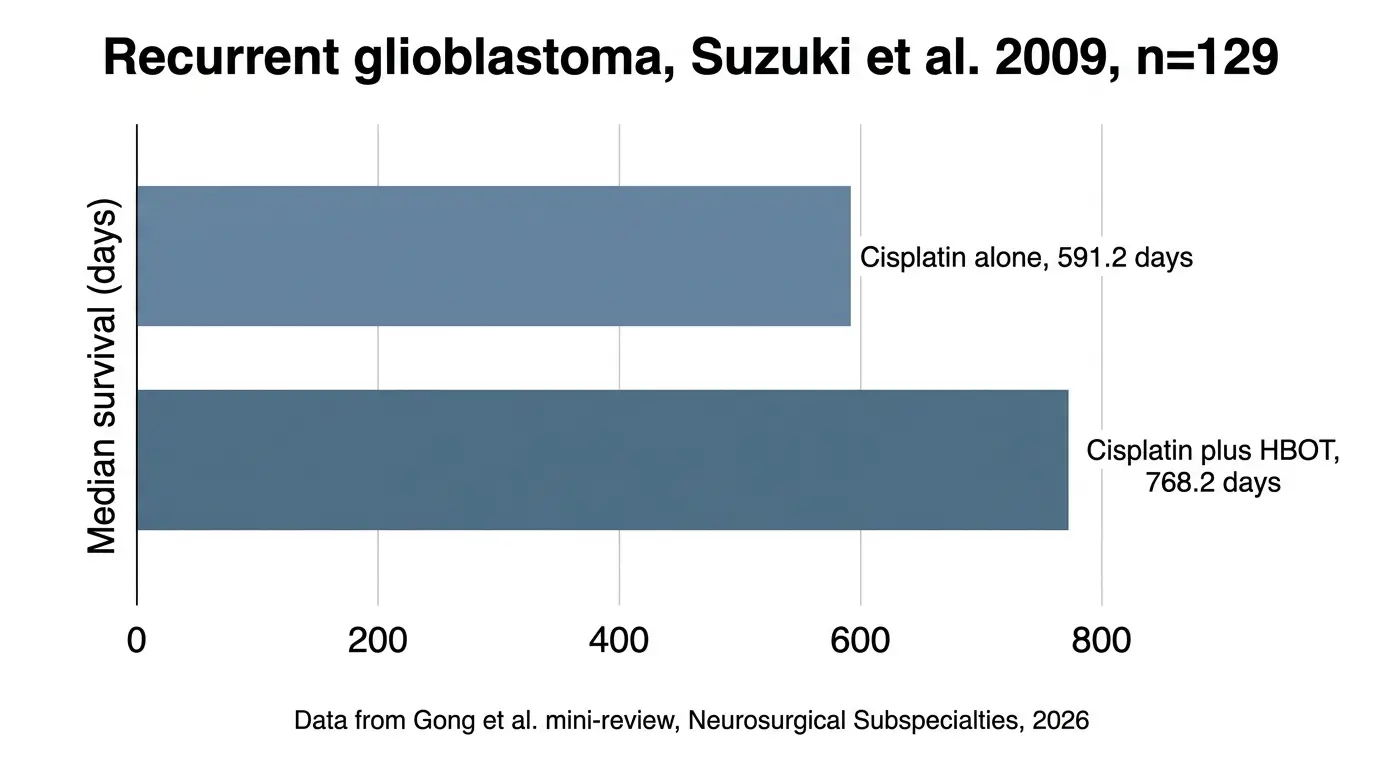
- One 129-patient study cited in the review reported median survival of 768.2 days for cisplatin plus hyperbaric oxygen versus 591.2 days for cisplatin alone.
- The same oxygen exposure can activate HIF, NF-kB and VEGF pathways that help tumor cells survive and grow.
- The authors call current clinical evidence immature and ask for multicenter randomized trials with standardized protocols.
Hyperbaric oxygen therapy can both sensitize glioblastoma to radiation and chemotherapy and, under some conditions, accelerate tumor growth, according to a peer-reviewed mini-review published 28 March 2026 in Neurosurgical Subspecialties.
The review, led by Sheng Gong and colleagues at the Department of Neurosurgery, Union Hospital of Tongji Medical College, Huazhong University of Science and Technology, synthesizes preclinical and small clinical studies of hyperbaric oxygen therapy (HBOT) in glioblastoma, the most common and aggressive primary brain tumor.
Standard care of surgery, radiotherapy and temozolomide leaves high recurrence rates, the authors wrote, and tumor hypoxia is a key driver of that resistance.
HBOT delivers 100 percent oxygen at 1.5 to 3.0 atmospheres absolute, which raises oxygen dissolved in plasma and pushes more oxygen into hypoxic tissue. Oxygen levels in glioblastoma tissue are generally below 5 percent and can fall below 0.1 percent in necrotic core regions, the review reported, citing earlier work.
On the anti-tumor side, the authors reported that HBOT raises tumor oxygen levels by 100 to 115 percent, which increases reactive oxygen species and DNA double-strand breaks during radiotherapy.
A 2022 study cited in the review found that HBOT combined with radiotherapy produced greater proliferation inhibition and higher apoptosis in U251 glioma cells than radiotherapy alone, according to Ma and colleagues.
For chemotherapy, the review cited a 2016 study by Lu and colleagues showing that HBOT enhanced the effect of nimustine in part by lowering hypoxia-inducible factor 1-alpha (HIF-1-alpha), tumor necrosis factor-alpha, interleukin-1-beta, vascular endothelial growth factor (VEGF), matrix metalloprotease 9 and nuclear factor kappa B (NF-kB).
HBOT also downregulated cancer stem cell markers CD133, CD15 and SOX2 in several cited studies, reducing self-renewal capacity.
The review then laid out the opposing evidence. Wang and colleagues, in a 2018 study cited by the authors, reported that HBOT at 2.4 atmospheres absolute promoted growth of GL261-Luc tumors and reduced necrosis in a C57BL/6J mouse model.
Ding and colleagues observed larger tumor volumes in Sprague-Dawley rats with glioblastoma xenografts after HBOT at 3.0 atmospheres absolute.
The authors identified two mechanisms behind the pro-tumor signal. Elevated reactive oxygen species can cause DNA damage and epigenetic changes that raise mutation rates.
HBOT can also stabilize HIF-1-alpha through nitric oxide signaling, increasing VEGF and basic fibroblast growth factor and supporting angiogenesis, according to work by Yamamoto and colleagues cited in the review.
Clinical evidence is limited and mixed. The review cited a 2009 study by Suzuki and colleagues of 129 patients in which the HBOT plus cisplatin group reached a median survival of 768.2 days, compared with 591.2 days for cisplatin alone.
Ogawa and colleagues reported in 2012 that 57 high-grade glioma patients receiving HBOT followed by radiotherapy and PCV chemotherapy had longer median survival than historical controls. Kohshi and colleagues reported better tumor regression in patients receiving HBOT with radiotherapy in a 1996 study of 21 patients.
The authors flagged clear limits to that evidence. Most clinical studies are small, non-randomized and use a single set of HBOT parameters without patient subgrouping. The review itself does not quantitatively synthesize the data, which the authors said may introduce selection bias.
Gong and colleagues call for multicenter randomized controlled trials with standardized HBOT regimens and biomarker-driven patient selection, using markers such as HIF-1-alpha, carbonic anhydrase IX, IDH mutation status, MGMT promoter methylation and stem cell markers CD133, CD15 and SOX2. They also propose testing HBOT alongside immune checkpoint inhibitors, targeted agents including N-acetylcysteine, and Tumor Treating Fields.
The work was funded by the Natural Science Foundation of China (grant 82473430), the Natural Science Foundation of Chongqing and the Chongqing Talent Program. The authors declared no conflicts of interest.
References
- Gong S, Liao B, Zhao L, Liu J, Wu N, Wang P. Dual Effects and Clinical Application Prospects of Hyperbaric Oxygen Therapy in Glioblastoma: A Mini Review. Neurosurgical Subspecialties, 28 March 2026. DOI: 10.14218/NSSS.2025.00047. https://www.xiahepublishing.com/3067-6150/NSSS-2025-00047
- Xia & He Publishing Inc. Dual effects and clinical application prospects of hyperbaric oxygen therapy in glioblastoma. EurekAlert! news release, 23 April 2026. https://www.eurekalert.org/news-releases/1124909