- A prospective cohort of 117 pregnant women with fetal growth restriction compared three treatment regimens at the Second Nanning People’s Hospital between July 2022 and June 2025.
- Patients receiving normobaric high-flow oxygen therapy plus low molecular weight heparin had a median neonatal birth weight of 2,600 grams, compared with 2,360 grams in the standard care group (P < 0.001).
- The fetal growth restriction cure rate reached 45.83 percent in the combined therapy group versus 18.75 percent in the standard care group (OR 3.67, 95 percent CI 1.21 to 11.15; P = 0.042).
- Low birth weight incidence fell to 33.33 percent in the combined therapy group, compared with 65.63 percent in the standard care group (P = 0.013).
- Preterm birth rates and umbilical artery blood gas values (pH, lactate) showed no significant differences across the three groups.
NANNING, China, May 20, 2026. Researchers at the Second Nanning People’s Hospital reported that combining normobaric high-flow oxygen therapy with low molecular weight heparin produced higher birth weights and a higher cure rate in pregnancies complicated by fetal growth restriction, according to a prospective cohort study published in the International Journal of Women’s Health.
The findings matter because fetal growth restriction is the second leading cause of perinatal mortality and affects about 8.77 percent of pregnancies in China, with limited evidence supporting standard interventions such as low-flow oxygen, nutritional supplementation, or vitamins. The study reported a 27 percentage point gap in cure rate between the combined therapy group and the standard care group, with an odds ratio of 3.67 (95 percent CI 1.21 to 11.15; P = 0.042).
Study design
The single-center prospective cohort study enrolled 117 pregnant women diagnosed with fetal growth restriction between July 2022 and June 2025. Treatment assignment used a non-randomized, patient-preference design rather than randomization, with shared decision-making between clinicians and patients.
Inclusion required a singleton viable pregnancy, gestational age between 28 and 37 weeks, idiopathic fetal growth restriction without other comorbidities, and written informed consent. Patients with diabetes, hypertensive disorders of pregnancy, fetal chromosomal abnormalities, or severe organ dysfunction were excluded.
The cohort included 52 cases of early-onset fetal growth restriction (diagnosed before 32 weeks) and 65 cases diagnosed at 32 weeks or later. Baseline characteristics, including maternal age, parity, pre-pregnancy body mass index, and umbilical artery Doppler indices, showed no significant differences across the three groups (P > 0.05).
Treatment protocols
Group 1, with 32 patients, received low-flow nasal oxygen at 2 to 5 L/min with 30 to 40 percent oxygen concentration, administered twice daily for 30 minutes per session over seven days. The group also received intravenous vitamin C in 5 percent glucose solution and 200 mL of compound amino acids daily for seven days.
Group 2, with 37 patients, received the Group 1 regimen plus subcutaneous low molecular weight heparin at 4,000 IU.
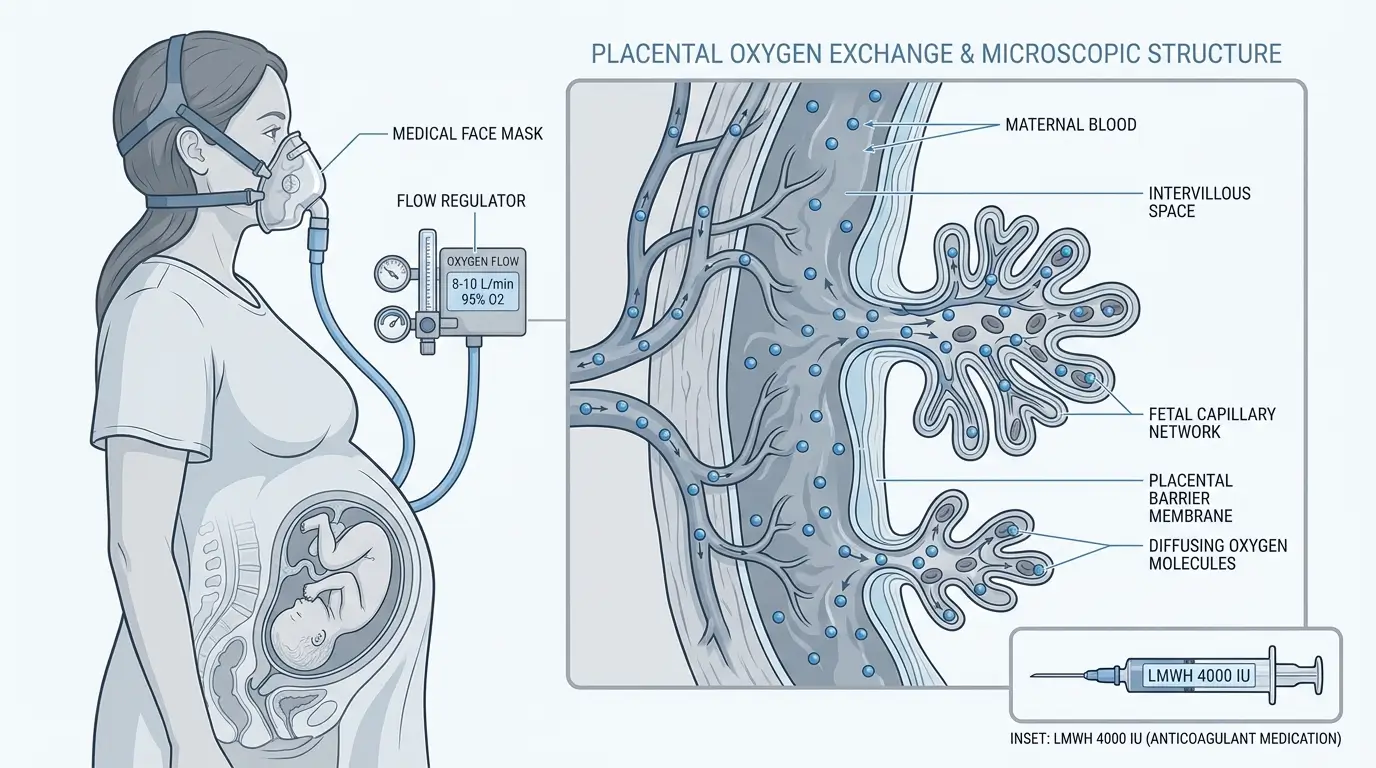
Group 3, with 48 patients, received the Group 2 regimen plus normobaric high-flow oxygen therapy. The high-flow protocol delivered 95 percent oxygen at 8 to 10 L/min through a sealed high-pressure mask outside a hyperbaric chamber, for 45 minutes once daily.
Primary outcomes
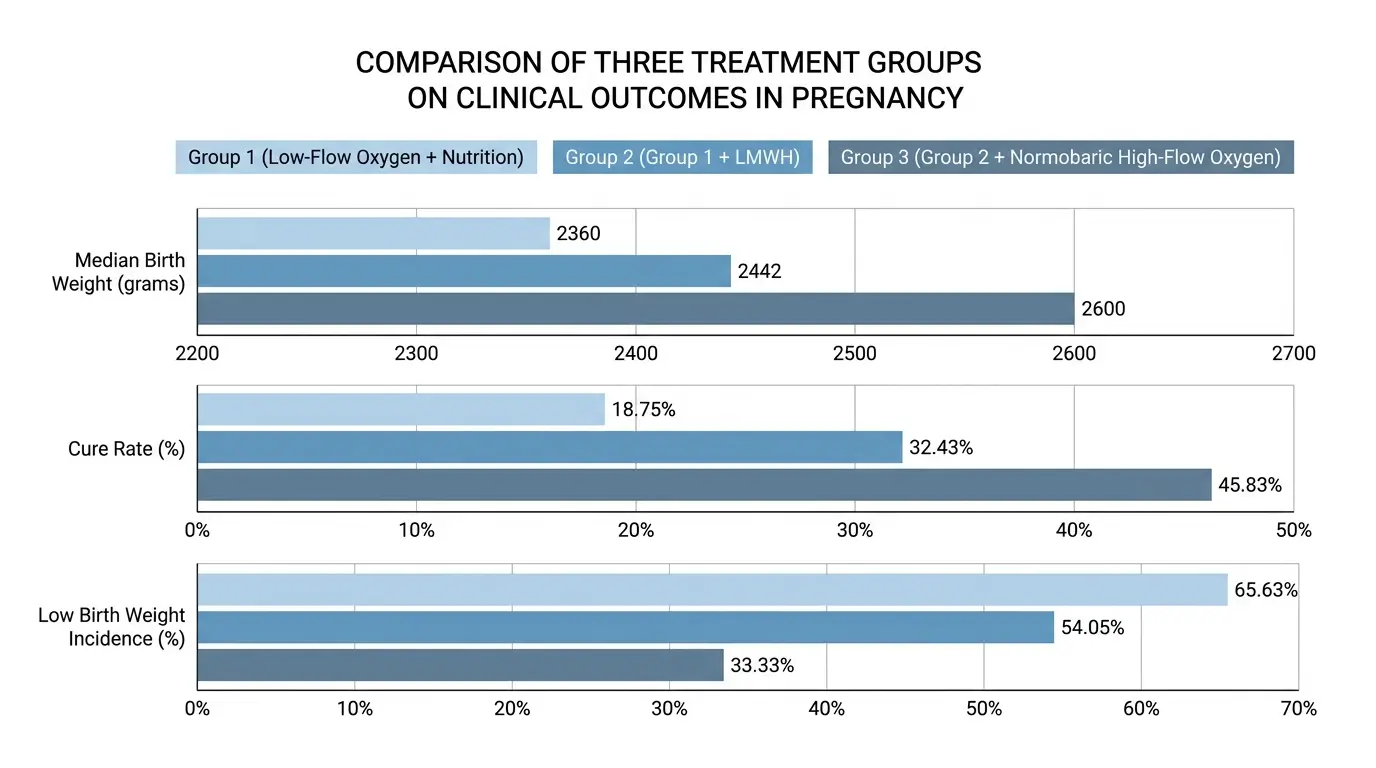
Median gestational age at delivery reached 267.5 days in Group 3, compared with 265.0 days in Group 1 and 264.0 days in Group 2 (overall P = 0.002). The difference between Group 1 and Group 2 was not statistically significant.
Median neonatal birth weight rose to 2,600 grams in Group 3, versus 2,442 grams in Group 2 and 2,360 grams in Group 1 (overall P < 0.001). The difference between Group 3 and Group 1 reached statistical significance, while Group 2 did not differ significantly from either group.
The fetal growth restriction cure rate, defined as birth weight at or above the 10th percentile for gestational age, reached 45.83 percent in Group 3 and 18.75 percent in Group 1 (P = 0.042). The Group 2 cure rate of 32.43 percent did not differ significantly from either other group.
Low birth weight incidence was 33.33 percent in Group 3, 54.05 percent in Group 2, and 65.63 percent in Group 1, with the Group 3 versus Group 1 comparison reaching significance (OR 0.26, 95 percent CI 0.09 to 0.74; P = 0.013).
Outcomes without significant differences
Preterm birth rates did not differ significantly across the three groups (P > 0.05). Umbilical artery blood gas parameters, including pH and lactate, also showed no significant differences. The authors noted that this suggests normobaric high-flow oxygen during pregnancy has limited effect on neonatal umbilical artery blood gas values.
Post-treatment umbilical blood flow Doppler parameters were not analyzed because follow-up timing varied across patients.
Additive rather than synergistic effect
The incremental benefit of adding normobaric high-flow oxygen to low molecular weight heparin alone (Group 3 versus Group 2) did not reach statistical significance for most endpoints. The cure rate comparison between these groups returned P = 0.213, although numerical trends favored Group 3.
The authors wrote that the combination “may yield additive rather than synergistic effects within this sample size, and larger studies are needed to detect smaller but clinically meaningful differences between these two active interventions.”
Proposed mechanism
The authors argued that normobaric high-flow oxygen therapy may offer a safety profile closer to standard care than hyperbaric oxygen therapy, while still raising maternal blood oxygen partial pressure and oxygen content. Hyperbaric oxygen therapy can raise blood oxygen partial pressure by 10 to 15 times and extend oxygen diffusion distance by 3 to 4 times, according to prior research cited in the paper.
The authors also referenced reported hyperbaric oxygen complications, including barotrauma-related middle ear damage at approximately 17 percent incidence and oxygen toxicity at around 2 percent. They cited these figures to argue that normobaric high-flow oxygen could offer an alternative with fewer risks during pregnancy.
Low molecular weight heparin contributes by inhibiting coagulation factors, reducing blood viscosity, and improving placental microcirculation, the authors wrote, citing prior work on placental thromboinflammation by Singh and colleagues in Blood Advances.
Study limitations
The authors identified several constraints on the findings. The non-randomized, patient-preference design is susceptible to residual confounding from unmeasured variables such as nutritional intake, gestational weight gain, maternal anemia, hypoalbuminemia, and subclinical antenatal infections.
The single-center setting and sample size of 117 limited statistical power and precluded multivariate adjustment. The cohort included both early-onset and late-onset fetal growth restriction subtypes, which differ in severity and placental pathophysiology, so the results represent an average effect across the spectrum.
The clinical significance of the observed increase in birth weight requires further evaluation, since long-term implications for child health were not assessed. Umbilical artery Doppler indices were compared as raw values rather than as proportions exceeding gestational age-specific thresholds.
What happens next
The authors called for large-scale randomized controlled trials with comprehensive phenotyping and long-term follow-up to confirm the efficacy of the combined regimen and identify which patient subgroups benefit most. They specified that future studies should monitor post-treatment umbilical blood flow parameters at fixed time points to address a methodological gap in the current work.
The study received approval from the Ethics Committee of the Second Nanning People’s Hospital (Approval No. Y2022021) and was registered with the Chinese National Medical Research Registration Information System (Registration No. MR-45-22-008098). Funding came from the Self-funded Research Project of the Health Commission of Guangxi Zhuang Autonomous Region (grant Z-A20221158). The authors declared no conflicts of interest.
References
- International Journal of Women’s Health (Dove Press). He M, Zhao K, et al. Efficacy of normobaric high-flow oxygen therapy combined with low molecular weight heparin in fetal growth restriction. https://www.dovepress.com/efficacy-of-normobaric-high-flow-oxygen-therapy-combined-with-low-mole-peer-reviewed-fulltext-article-IJWH
- Blood Advances. Singh KK, Gupta A, Forstner D, et al. LMWH prevents thromboinflammation in the placenta via HBEGF-AKT signaling. 2024;8(18):4756-4766. https://doi.org/10.1182/bloodadvances.2023011895