- A 62-year-old Canadian woman developed multiple rib fractures after receiving breast cancer radiotherapy twice over 17 years. Conservative treatment with medication and hyperbaric oxygen therapy (HBOT) healed her bones without surgery.
- Breast cancer survivors now live longer. Radiation exposure from repeat treatments is increasing. Clinicians may see more cases of osteoradionecrosis, a rare but serious complication.
- The woman returned to playing tennis after seven weeks of HBOT.
- Her cumulative radiation dose exceeded 8,700 cGy, well above the 6,000 cGy threshold linked to osteoradionecrosis risk.
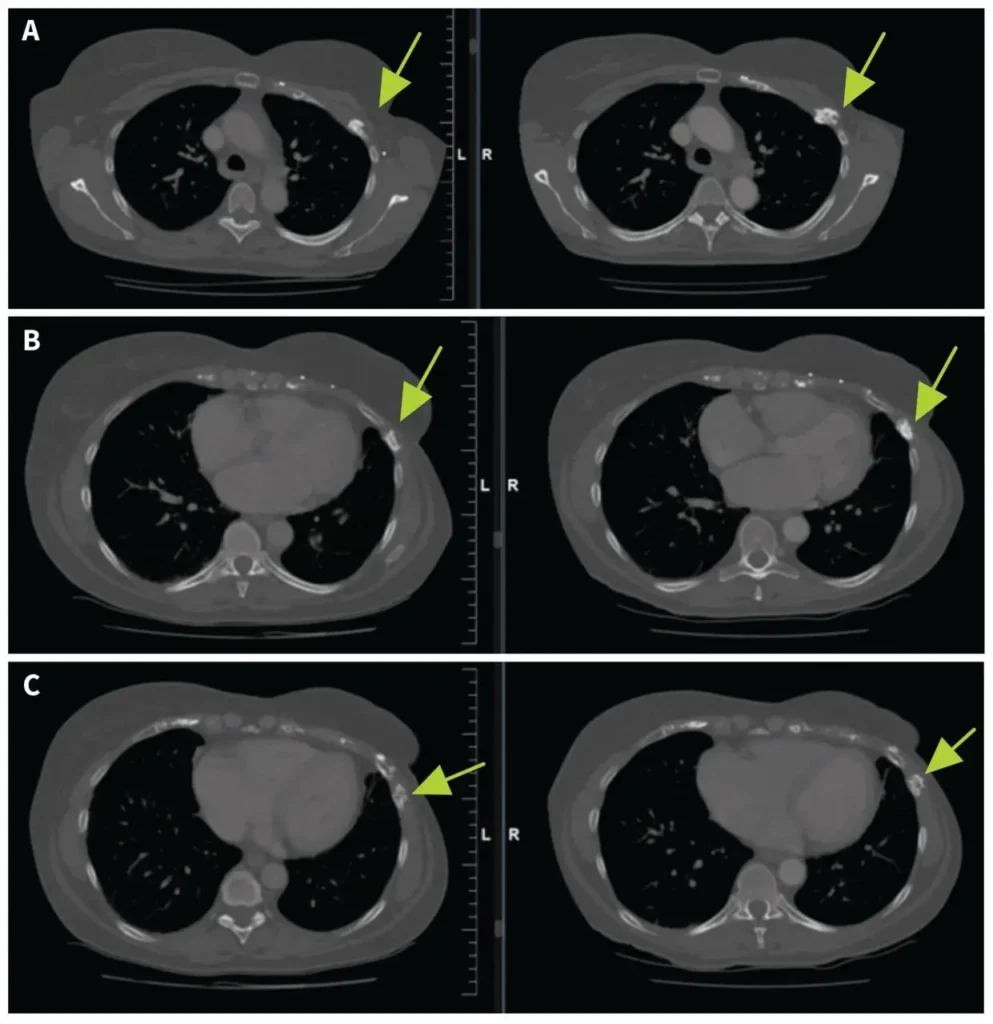
- CT scans showed healing in ribs 3 through 7 after 11 months of follow-up.
A case report published in the Canadian Medical Association Journal in September 2025 describes a 62-year-old woman who developed osteoradionecrosis (ORN) after receiving breast radiotherapy at two different points in her life. The condition caused multiple rib fractures on her left side.
Physicians successfully treated her with a combination of pharmacotherapy and hyperbaric oxygen therapy, avoiding surgery.
The patient was first diagnosed with early-stage breast cancer at age 35. She underwent a lumpectomy, axillary lymph node dissection, and adjuvant radiotherapy using a Cobalt-60 unit. Her total dose at that time included 4,000 cGy to the left breast and an additional 1,250 cGy boost to her breast scar.
Seventeen years later, at age 52, she experienced a breast cancer recurrence. This second cancer was more aggressive, with extensive intraductal component and dermal lymphovascular invasion.
She received a left skin-sparing mastectomy with immediate reconstruction, adjuvant chemotherapy, and another course of radiotherapy. The second treatment delivered 4,500 cGy to the left chest wall and 5,000 cGy to regional lymph nodes.
Seven years after her recurrence, the woman began experiencing left chest discomfort. Her symptoms progressed over three years. CT imaging revealed fractures in her second through seventh ribs, with sclerosis, cortical irregularity, and callous formation. A radiologist flagged concerns for radiation-induced rib fractures from osteoradionecrosis.
Her estimated cumulative dose to the chest wall exceeded 8,700 cGy, with the lateral boost region receiving more than 10,000 cGy. These figures do not account for any tissue recovery during the 17-year gap between treatments.
What Is Osteoradionecrosis?
Osteoradionecrosis occurs when radiation damages blood vessels in bone tissue. The affected bone becomes hypovascular, hypocellular, and hypoxic. This leads to progressive tissue death and reduced healing capacity.
The condition is most common in the mandible after head and neck cancer treatment, where radiation doses are typically higher. In breast cancer patients, ORN of the ribs occurs in only 0.1% to 5% of cases involving chest wall irradiation.
Risk factors include cumulative doses above 6,000 cGy, repeat irradiation, trauma, infection, and individual sensitivity to radiation damage.
Treatment Approach
The patient was referred to an Adult Radiation Late Effects Clinic. Physicians started her on a combination of pentoxifylline 400 mg twice daily, vitamin E 1,000 IU daily, and pravastatin 40 mg daily. She continued calcium and vitamin D supplementation.
Pentoxifylline is an anti-inflammatory vasodilator that decreases blood viscosity and improves oxygen delivery to hypoxic tissues. Vitamin E (tocopherol) is an antioxidant that protects cells from reactive oxygen species. Research suggests these drugs have a synergistic effect when used together.
Statins have also shown promise in managing radiation-induced toxicity. A study by Kusumoto and colleagues found that statin exposure was a favorable prognostic factor for osteoradionecrosis of the mandible, with an adjusted hazard ratio of 3.71.
The patient reported improvement in pain as early as two weeks after starting pharmacotherapy. She tolerated the medications well, with no signs of toxicity on blood tests.
Hyperbaric Oxygen Therapy
After initial drug treatment, the patient completed eight weeks of HBOT. This therapy involves breathing pure oxygen in a pressurized chamber. The theorized mechanism is promotion of angiogenesis, or new blood vessel formation, in hypoxic tissues.
A 2024 randomized controlled trial published in JAMA Oncology found that 6 to 8 weeks of HBOT yielded significant reductions in pain and fibrosis in women experiencing late toxic effects from irradiated breast cancer.
The patient developed myopia during HBOT, a known side effect. This required only contact lenses, not specific treatment. After seven weeks of therapy, she returned to physical activities, including tennis.
(Ed. note: The fact that she resumed tennis after just seven weeks of HBOT demonstrates how effective conservative management can be for this condition.)
CT imaging performed 11 months after her baseline scan showed interval healing of ribs 3 through 7, with no new lucencies or fractures. She subsequently reduced her pentoxifylline dose to 400 mg once daily while maintaining her response.
Clinical Implications
No universal guidelines exist for screening breast cancer patients for osteoradionecrosis. However, the case report authors suggest that patients receiving cumulative doses above 6,000 cGy should be considered for closer monitoring.
The Common Terminology Criteria for Adverse Events grades osteoradionecrosis based on symptoms and functional limitations. Patients with imaging findings but no symptoms are classified as grade 1 and monitored without intervention.
Those with symptoms limiting instrumental activities of daily living are grade 2, and conservative medical management is recommended. Severe symptoms limiting self-care require grade 3 classification, where elective surgical intervention may be necessary.
In this case, surgical intervention was considered but not recommended by the consulting surgeon. The conservative approach proved effective.
Modern approaches to repeat radiation for breast cancer recurrence aim to minimize toxicity. Partial breast reirradiation, which targets only the lumpectomy cavity, has shown a 5-year recurrence rate of only 5% with minimal late grade 3 or higher toxicity.
(Ed. note: As breast cancer survival rates improve and reirradiation becomes more common, clinicians should expect to see more cases of osteoradionecrosis in the coming years.)
The case report was authored by Nicholas Lum and Jennifer Yin Yee Kwan of the University of Toronto. Kwan disclosed receiving research funding from The Princess Margaret Cancer Foundation and an American Association for Cancer Research award. The authors obtained patient consent for publication.
References
- Lum N, Kwan JYY. Osteoradionecrosis secondary to breast reirradiation. CMAJ. 2025;197(31):E1000-E1003. https://doi.org/10.1503/cmaj.250402
- Mink van der Molen DR, Batenburg MCT, Maarse W, et al. Hyperbaric oxygen therapy and late local toxic effects in patients with irradiated breast cancer: a randomized clinical trial. JAMA Oncol. 2024;10:464-474
- Kusumoto J, Muraki Y, Sakakibara A, et al. Effect of statins on patients with osteoradionecrosis of the jaw. J Oral Maxillofac Surg. 2024;82:1585-1595
- Arthur DW, Winter KA, Kuerer HM, et al. Effectiveness of breast-conserving surgery and 3-dimensional conformal partial breast reirradiation for recurrence of breast cancer in the ipsilateral breast: the NRG Oncology/RTOG 1014 phase 2 clinical trial. JAMA Oncol. 2020;6:75-82.