- A patient with bile duct cancer at KBC Rijeka developed a severe duodenal ulcer 18 months after stereotactic body radiotherapy (SBRT), and doctors successfully treated it using hyperbaric oxygen therapy.
- No published data exist for this specific application, making it a potential global first.
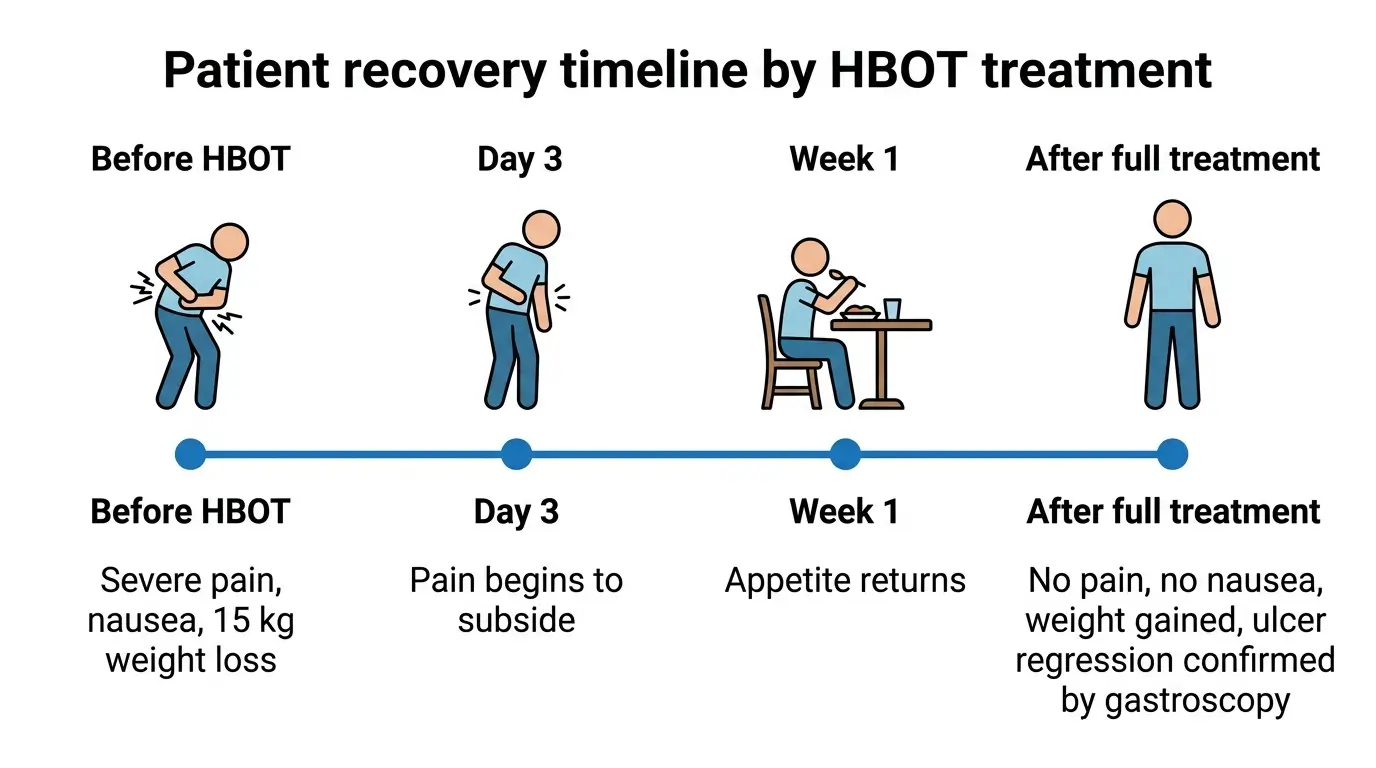
- The patient lost roughly 15 kilograms before treatment and could not continue cancer therapy.
- Improvements began within three days of starting hyperbaric oxygen sessions.
- A second patient with similar complications is already receiving the same treatment at KBC Rijeka.
Doctors at Clinical Hospital Centre Rijeka (KBC Rijeka) in Croatia have reported what they believe is the first successful use of hyperbaric oxygen therapy (HBOT) to treat severe gastrointestinal complications caused by stereotactic body radiotherapy (SBRT). The case, announced on April 2, 2026, involved a patient with bile duct cancer whose condition had stopped responding to conventional medication.
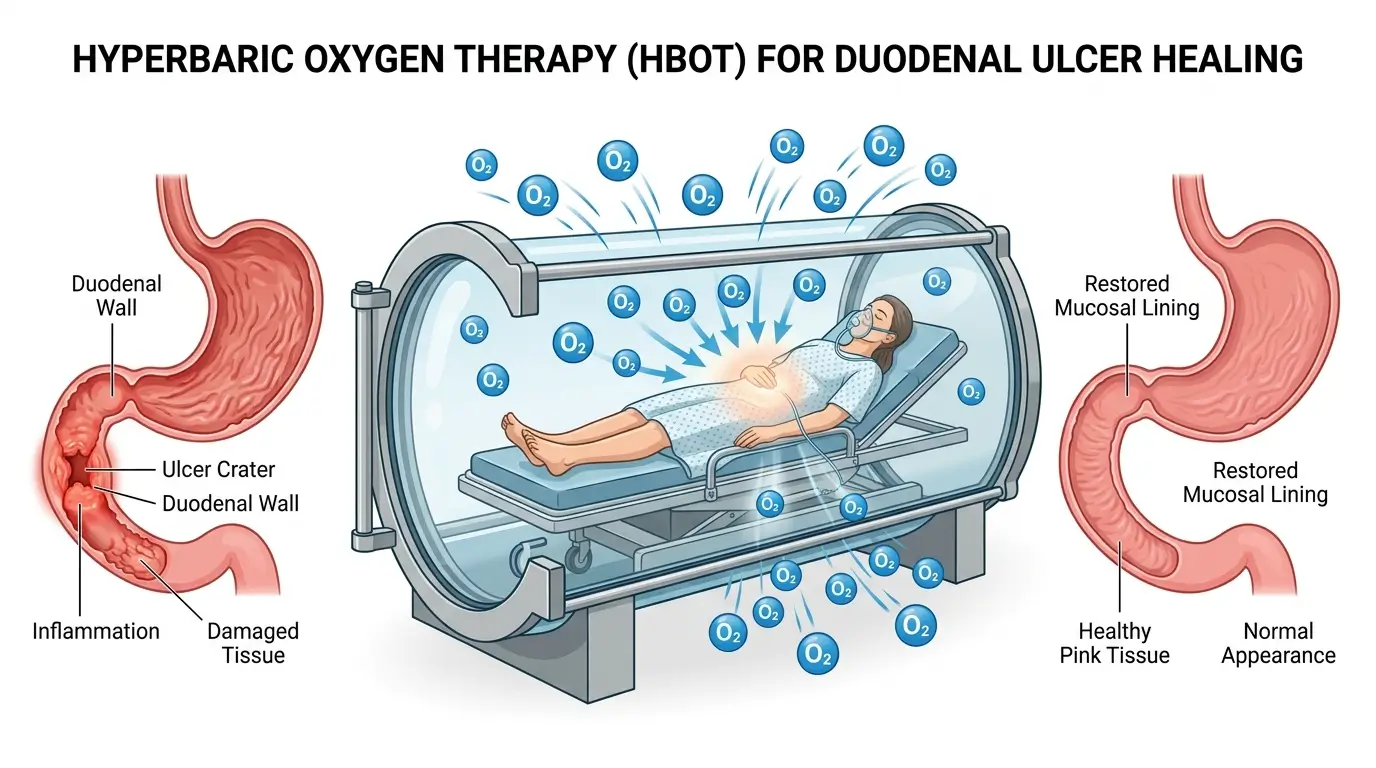
The patient had originally received SBRT to treat liver metastases at another medical institution. About 18 months later, a large ulcer developed in the descending duodenum. That ulcer brought severe abdominal pain, persistent nausea, and significant weight loss of around 15 kilograms. The symptoms were serious enough to halt the patient’s ongoing cancer treatment.
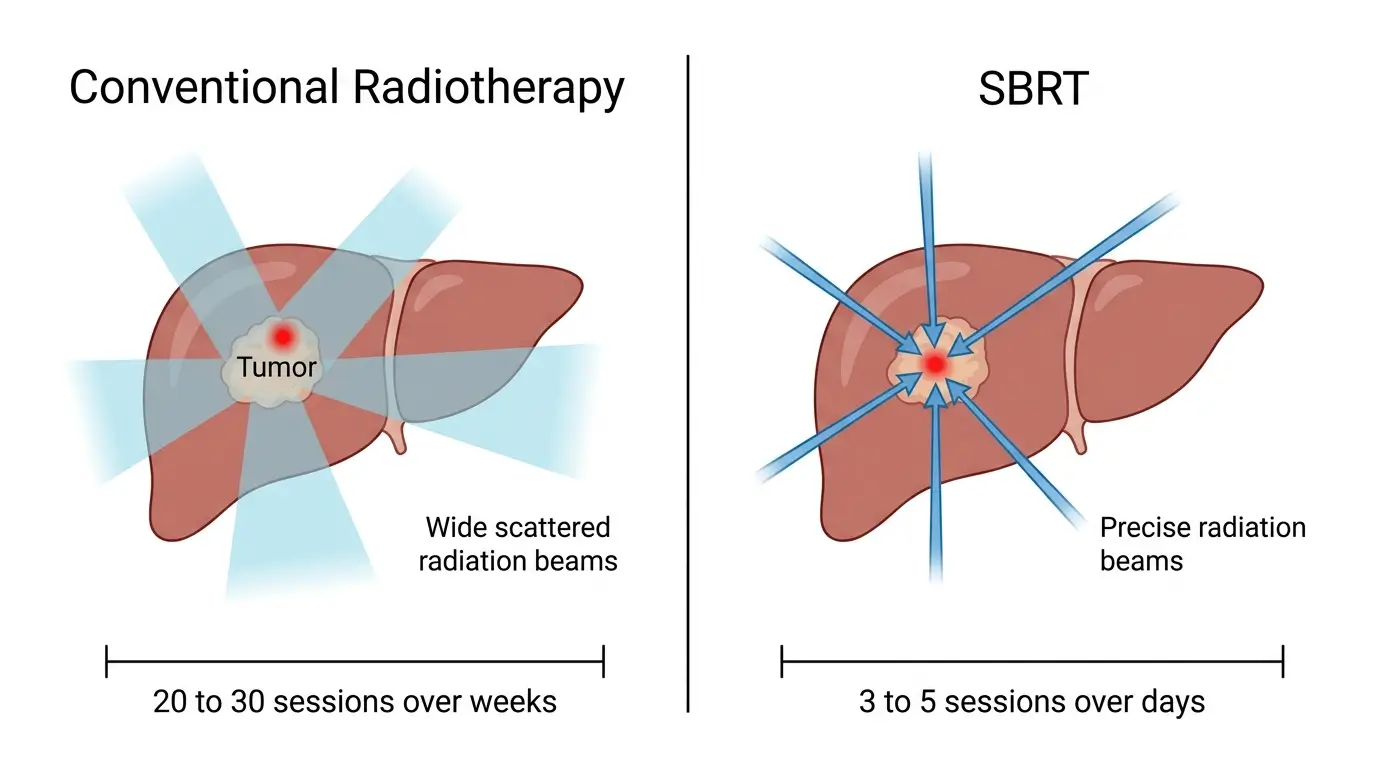
SBRT is a radiation technique that delivers high doses of targeted radiation to tumors in fewer sessions than conventional radiotherapy. It is increasingly used for primary and metastatic tumors in the liver, pancreas, adrenal glands, and abdominal lymph nodes. The precision of SBRT limits damage to surrounding healthy tissue, but late side effects can still emerge, sometimes months or years after treatment.
When standard medications failed to heal the ulcer, the medical team at KBC Rijeka turned to HBOT. The treatment places patients in a pressurized chamber where they breathe pure oxygen. It has an established track record in treating radiation injuries, chronic wounds, and certain bone conditions. A clinically focused review published in CA: A Cancer Journal for Clinicians in December 2025 confirmed that HBOT is “the only intervention known to provide symptom relief through disease modification” for late radiation-induced effects. The same review noted that an estimated 5% to 10% of patients who receive radiotherapy will eventually develop severe late effects.
The distinction in the Rijeka case is the type of radiation involved. While some studies support HBOT for complications from conventional radiotherapy affecting the digestive system, the hospital says there are currently no published data showing its effectiveness for complications specifically caused by SBRT in the abdomen and pelvis.
Professor Ivana Mikolasevic, head of the oncology clinic at KBC Rijeka, described the results. “After the therapy, the patient no longer experiences pain or nausea, has gained significant weight, and follow-up gastroscopy shows a clear regression of the duodenal ulcer,” she said.
Doctors reported that improvement began after three days of treatment. Pain subsided and appetite returned within the first week.
The hospital’s hyperbaric medicine department is currently the only center in Croatia fully equipped to treat critically ill patients with HBOT. Treatment cycles at the facility run between 20 and 60 sessions, administered five days per week. The team is led by specialist Mario Franolic.
The absence of any published literature on HBOT for SBRT-related abdominal complications makes this case especially significant for oncologists managing the growing population of long-term SBRT survivors.)
A 2025 safety evaluation published in Medicina analyzed 45 cancer patients who received HBOT and found no evidence that the therapy contributes to tumor progression, recurrence, or metastasis. That study, conducted at Gulhane Research and Hyperbaric Medicine Hospital, reported that 59.5% of patients experienced no cancer recurrence during a median follow-up of 783 days. The statistical analysis showed no significant correlation between the number of HBOT sessions and either mortality (p = 0.881) or metastasis (p = 0.213).
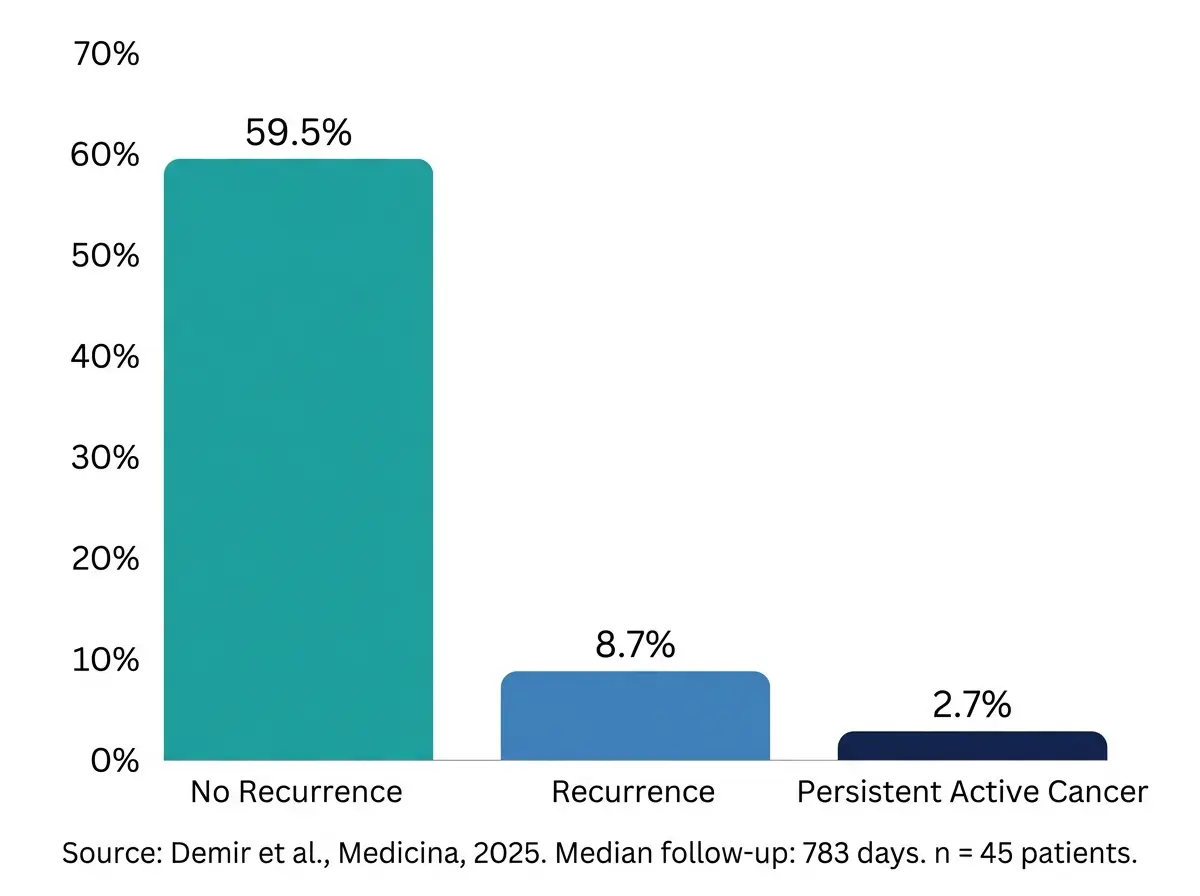
This safety profile matters because cancer patients and their doctors have historically worried about whether breathing pure oxygen under pressure might stimulate tumor growth. The Medicina study’s authors concluded that “HBOT appears to be a safe and effective adjunctive therapy for managing complications in patients with solid tumors.”
The Rijeka case also reflects a broader shift in oncology. As cancer patients live longer, managing the late side effects of aggressive treatments like SBRT has become a growing concern. The December 2025 review in CA: A Cancer Journal for Clinicians noted that the number of cancer survivors in the United States is projected to exceed 22 million by 2030. Many of these survivors will face chronic, sometimes debilitating complications from prior radiation treatment.
HBOT works by increasing the partial pressure of oxygen in the blood, which promotes new blood vessel formation, activates fibroblasts, reduces tissue swelling, and shifts immune responses toward tissue repair. According to the 2017 European Consensus Conference on Hyperbaric Medicine, HBOT is recommended for 22 distinct indications, six of which are related to radiotherapy.
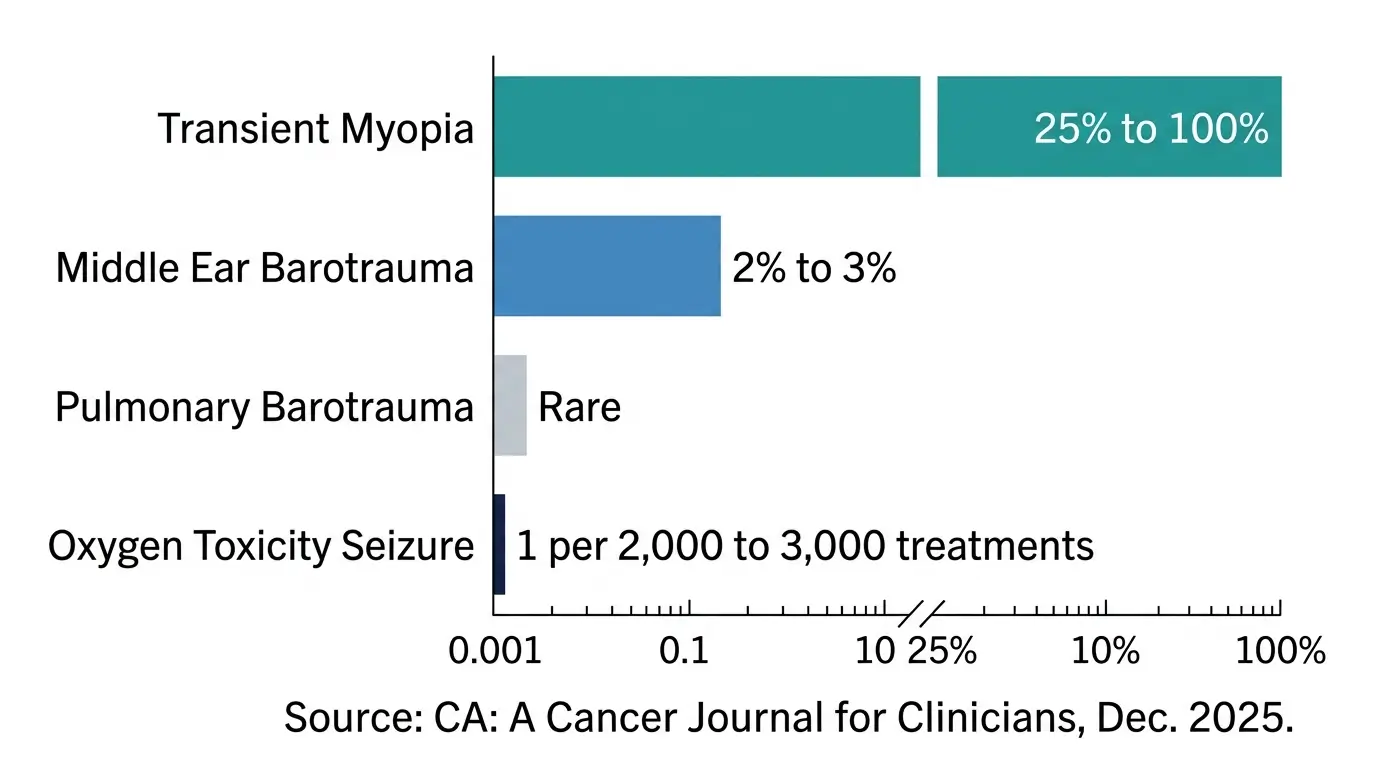
Standard HBOT protocols involve delivering medical-grade oxygen (above 99% purity) at 1.9 to 6.0 atmospheres absolute for 90 to 120 minutes per session. Side effects are generally mild. The most common include transient myopia (25% to 100% of patients, depending on definition) and minor middle ear barotrauma (2% to 3%). Oxygen toxicity seizures are rare, occurring in roughly one per 2,000 to 3,000 treatments.
Following the success of the first case, a second patient with similar SBRT-related complications is already undergoing HBOT at KBC Rijeka. The hospital says the results highlight the value of multidisciplinary collaboration between its oncology clinic, hyperbaric medicine department, and broader care teams.
Whether this single case leads to broader adoption will depend on formal publication in peer-reviewed journals and replication at other institutions. For now, it represents a concrete data point for clinicians weighing treatment options when SBRT patients develop late gastrointestinal injuries that resist conventional therapy.
References
- Croatia Week. “Croatian doctors achieve world-first success treating cancer therapy complications with oxygen therapy.” April 2, 2026. https://www.croatiaweek.com/croatia-rijeka-hyperbaric-oxygen-cancer-therapy-breakthrough/
- Mink van der Molen DR, et al. “Hyperbaric oxygen therapy for chronic radiotherapy-related adverse effects: A clinically focused review.” CA: A Cancer Journal for Clinicians. December 12, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12700310/
- Demir KC, et al. “Hyperbaric Oxygen Therapy for Managing Cancer Treatment Complications: A Safety Evaluation.” Medicina. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11943617/